Summary
- In Ontario, the number of new HIV diagnoses has increased in recent years. Challenges to interpreting diagnosis trends include:
- The double-counting of individuals diagnosed through anonymous testing (duplicate diagnoses).
- The inclusion of people who were diagnosed outside of the province and later moved to Ontario and tested again (‘out-of-province’ diagnoses).
- In recent analyses led by OHESI, removing duplicates decreased the number of diagnoses in 2017 from 935 to 916. Also removing ‘out-of-province’ diagnoses further reduced this number to 797.
- These analyses also suggest that the overall increase in new diagnoses between 2016 and 2017 was the result of an increase in ‘out-of-province’ diagnoses, rather than an increase in new HIV transmissions in the province.
Surveillance data on new HIV diagnoses are often used by front-line service providers and policy makers to inform their work. Information collected on diagnoses, such as sociodemographics and HIV risk factors, is commonly used to:
- guide the planning and delivery of appropriate HIV care.
- inform HIV prevention initiatives and evaluate their success (as new diagnoses are often used as an indirect way of measuring new infections).
This blog post describes the challenges of using Ontario surveillance data for the above purposes, OHESI’s recent work in refining these data and the impact of these refinements on recent trends.
Information collected during HIV testing in Ontario
Before discussing refinements to HIV surveillance, it is important to understand the HIV testing process and how information on newly diagnosed individuals is collected in Ontario.
When a person is tested for HIV in the province, the health care provider ordering the test fills out an HIV test requisition form. This form collects information on the person tested, including sex, date/year of birth, HIV risk factors and either the person’s name (nominal testing) or an anonymous code (anonymous testing).
When a person tests positive for HIV, Public Health Ontario sends a second form – the Laboratory Enhancement Program (LEP) questionnaire – to the health care provider who ordered the initial test. The purpose of this second form is to supplement the HIV test requisition and provide a more comprehensive understanding of who is being diagnosed with HIV in Ontario. Data collected on the LEP form includes some of the same information documented on the requisition form, as well as other information, such as race/ethnicity, country of birth and HIV testing history.[1]
Double-counting of diagnoses
In Ontario, a new diagnosis is defined as an individual’s first HIV-positive test result in the province. This means that if a person receives more than one HIV-positive test in Ontario (see Box below), only the first test is counted as a new diagnosis in order to avoid double-counting. Duplicate diagnoses are identified and removed when test information is entered into the laboratory surveillance databases at Public Health Ontario.
Why might a second HIV diagnostic test be conducted?
There are several possible reasons. For example, some physicians order an HIV test to confirm an individual’s diagnosis when the person first enters care.
Anonymous testing provides an important option for people concerned about privacy; however, it complicates the accurate collection of surveillance information and can result in an individual being counted twice in the data. With anonymous testing, duplicate diagnoses are difficult to identify due to the lack of identifying information collected on the person tested. For example, someone who initially received an HIV-positive diagnosis through anonymous testing, and later had a nominal HIV test when entering care, may be counted twice as a new diagnosis.[2] Individuals who receive more than one anonymous HIV-positive test may also be counted twice.
When people are double-counted, the number of new diagnoses included in Ontario surveillance reports is higher than the actual number of diagnoses.
‘Out-of-province’ diagnoses
Interpretation of diagnosis trends is also complicated by individuals who were initially diagnosed outside of Ontario and then moved to the province and tested for HIV again (for example, as part of the immigration process or when entering care). These ‘out-of-province’ diagnoses are counted as a new diagnosis in Ontario and their inclusion means that trends can be influenced by migration patterns to the province, in addition to other factors. This makes it difficult to interpret trends. For example, an increase in new diagnoses could be due to more HIV transmissions occurring in Ontario, more HIV-diagnosed individuals moving to and being re-tested in Ontario, or a combination of both.
Refining Ontario’s HIV surveillance data
OHESI (a collaboration between Public Health Ontario and the Ontario HIV Treatment Network, AIDS Bureau of the Ontario Ministry of Health and Long-Term Care, and Public Health Agency of Canada) is dedicated to providing the best possible provincial surveillance numbers for Ontario. By refining the new diagnosis data, we may be able to better estimate the actual number of people who receive a first time HIV-positive diagnosis in Ontario, as well as improve our ability to interpret trends.
Recently, OHESI conducted new analyses to determine how information collected on HIV testing history (on the LEP form) could help improve these data. This LEP-based information includes when and where an individual has previously tested positive for HIV.[3]
In these new analyses:
- diagnoses with history of a previous HIV-positive test result within Ontario were removed in order to reduce double-counting (as these diagnoses are duplicates and would have already been counted as a new diagnosis with their first positive test in Ontario).
- individuals with history of a previous HIV-positive test result outside of Ontario (‘out-of-province diagnoses) were removed in order to better assess trends in new HIV infections that occurred in the province (as these individuals were most likely infected with HIV outside of Ontario).
Note: Diagnoses with history of a previous HIV-positive test result are referred to as ‘previous positives’ in the remainder of this post.
What is the impact of removing previous positives?
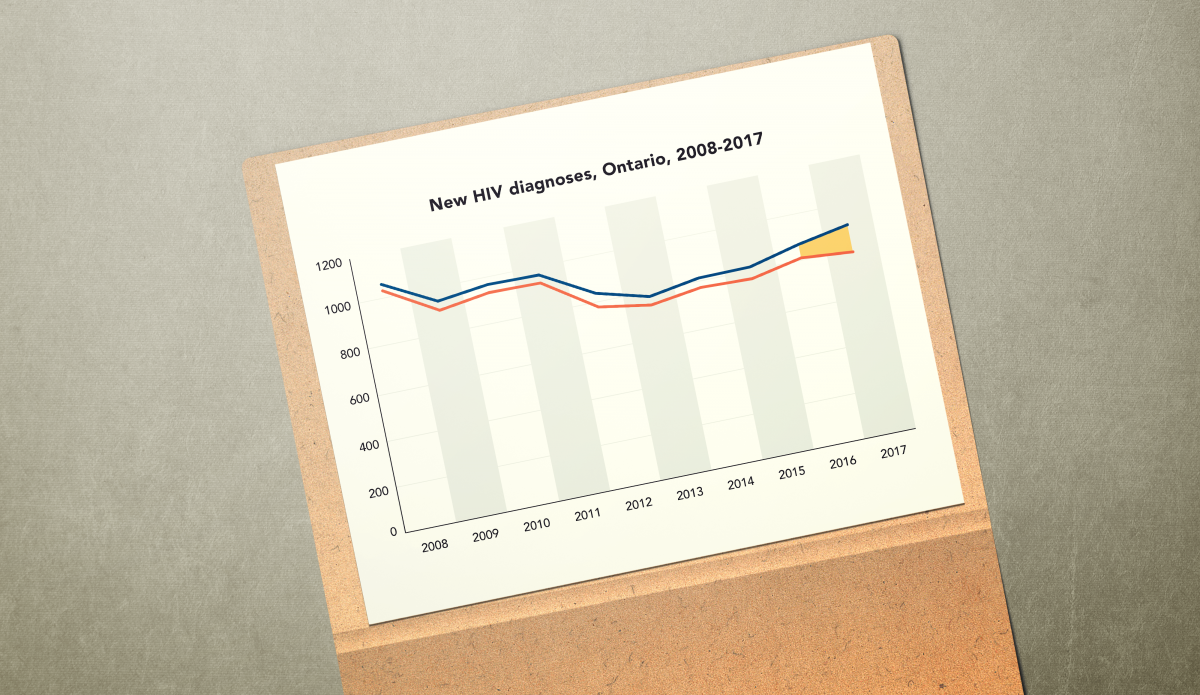
Trends in the number of new diagnoses in Ontario between 2008 and 2017 are shown in the figure below, along with the impact of excluding previous positives.

The top line displays the trend in new diagnoses when the LEP is not used to remove any previous positives. This line shows a decrease in diagnoses in the earlier part of the past decade, followed by an increase between 2013 and 2017.
When the LEP form is used to address double-counting and remove duplicate diagnoses with history of a previous positive test result within Ontario (the middle line), the trend is identical but there are an average of 22 fewer diagnoses each year.
When ‘out-of-province’ diagnoses are also removed (the bottom line), the difference is more noticeable. In this scenario, the trend is identical until 2016 and then – instead of continuing to increase – the number of new diagnoses in Ontario decreases to 797 in 2017.
Taken together, these data suggest that the increase in new diagnoses between 2016 and 2017 (as observed in the top and middle lines) was the result of an increase in ‘out-of-province’ diagnoses, rather than an increase in new HIV transmissions in the province. Further, these data suggest that the number of new HIV infections occurring in Ontario in recent years may be closer to 800 than 900, and possibly lower (information on HIV testing history is missing for about half of diagnoses each year).[4]
Implications
Moving forward, OHESI will use information collected on HIV testing history to refine Ontario diagnosis data.
Future OHESI knowledge exchange products will exclude diagnoses with history of a previous positive within Ontario to reduce double-counting. Importantly, OHESI will continue to include ‘out-of-province’ diagnoses to provide an accurate picture of how many people and who require HIV care in the province. However, in separate tables and figures, OHESI will also exclude ‘out-of-province’ diagnoses in order to better understand trends in new HIV infections and guide HIV prevention priorities.
We hope these refinements will enhance the usefulness of surveillance data for people working in HIV.
Footnotes